Stay Ahead of the Curve in Radiology AI.
RadAI Slice is your weekly intelligence briefing on the most critical developments at the intersection of radiology and artificial intelligence. Stop searching. Start leading.Subscribe to join 11k+ radiology professionals tracking the future of imaging AI.
Featured In

Lastest Issues
The latest developments in Radiology & AI.





Reports & Market Maps
Explore our deeper briefings on radiology AI trends, market structure, and event-level intelligence.

SIIM 2026 AI Landscape
Analysis of SIIM 2026 sessions, themes, speaker mix, and abstract activity through the lens of imaging AI.

ECR 2026 AI Product Landscape
A launch-level view of ECR 2026 product announcements: AI share, product mix, and modality focus.

ECR 2026 AI Industry Landscape
A data-driven map of ECR 2026 exhibitors: AI share, vendor mix, and regional patterns.
Your Weekly Slice of Innovation
Each issue is precisely structured to give you exactly what you need. No fluff, just facts and forward-looking insights.
Recent Industry News
The Latest Research
FDA Approvals Database
Latest News & Trends

AI Unlocks Hidden Brain Lesions in Multiple Sclerosis via MRI
AI-enabled image processing reveals invisible cortical lesions in MRI scans of MS patients, advancing diagnosis and research.
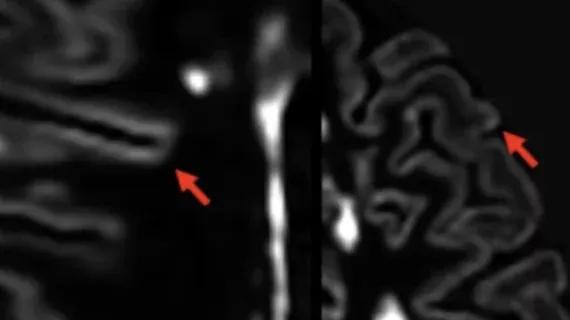
AI Technique Unveils Previously Hidden MS Gray Matter Lesions on MRI
Researchers developed an AI-enhanced method to detect previously invisible gray matter lesions in multiple sclerosis using MRI.

AI-Driven Molecular Profiling Enhances Thrombosis Risk Prediction
Researchers create an AI model integrating genetic, clinical, and transcriptomic data to identify individuals at risk for thrombosis.
From the Research Hub
FAA-Net: Fetal abdominal anomaly diagnosis in prenatal ultrasound via LLM-enhanced multi-instance learning.
As a critical prenatal screening tool, ultrasound (US) heavily depends on operator experience, leading to both challenging and rare fetal malformation diagnoses as well as diagnostic variability. Thus, developing an automated fetal anomaly detection system can reduce operator variability and expedite clinical analysis. Currently, most existing methods perform independent image-based predictions on different planes and use simple pooling strategies for case-level prediction, disregarding inter-image correlations. Although multi-instance learning (MIL) can model inter-image correlations, it suffers from attention dispersion as the number of images per case increases, limiting the model's ability to capture spatial and morphological differences across anomaly categories. To address these limitations, we propose FAA-Net for diagnosing fetal abdominal anomalies. (1) We introduce a Mixture of View Experts module that captures spatial features from specialized sub-expert networks. (2) We develop an LLM-Enhanced Feature Selection module that mines the rich medical knowledge embedded in LLMs to select diagnostically relevant images, enabling the model to better focus and capture category-specific patterns. (3) A simple attention mechanism is used to capture inter-image spatial and morphological correlations. Extensively validated on a multi-center prenatal fetal abdominal ultrasound dataset containing 2,732 cases (77,833 images across 5 categories) and the public TMED-2 dataset, our proposed FAA-Net outperforms state-of-the-art competitors. Code is available at: Github.
Machine learning-based prediction of non-ionic iodinated contrast media-induced acute adverse reactions following contrast-enhanced CT.
Iodinated contrast media (ICM) used in contrast-enhanced CT (CECT) examinations may induce acute adverse reactions (AAR) with different severity. To improve upon traditional linear risk assessments, this study aims to develop and validate a machine learning (ML)-based predictive model for ICM-AAR using routinely available clinical factors from a large-scale real-world cohort. Five ML models including Logistic Regression, Random Forest, XGBoost, CatBoost and LightGBM were trained and validated on a retrospective cohort of 332,090 patients who underwent CECT scans between 2014 and 2020. The final cohort was split into train, test and external validation datasets. Synthetic minority over-sampling technique (SMOTE) and under-sampling strategies were used to balance the data. Model training was performed using the GridsearchCV algorithm with 5-fold cross-validation. Model performance was evaluated using the area under the receiver operating characteristic curve (AUROC). The SHapley Additive exPlanations (SHAP) algorithm was performed to identify the most significant features. The train set included 132,102 patients (median age, 60 years [IQR, 49-69 years]; 72,666 males). The CatBoost model exhibited the best performance, with an AUROC of 0.6916 (95%CI = [0.6555, 0.7272]) in test set (n = 56,616; median age, 60 years [IQR, 49-69 years]; 31,400 males) and 0.6565 (95%CI = [0.6206, 0.6913]) in external validation set (n = 111,334; median age, 58 years [IQR, 49-68 years]; 61,447 males). Age, Injection rate, Type of contrast media, Injection dose, and Examination site were identified as the five most significant features by SHAP analysis. A ML model based on clinical factors was capable of predicting the occurrence of ICM-AAR, demonstrating improved ability in tackling extreme class imbalance. The model could be used to help clinical decision-making.
Leveraging Self-Supervised Learning for Non-Invasive Intra-Cardiac Magnetic Resonance Oximetry Assessment
Accurate measurement of intra-cardiac blood oxygen (O2) saturation is essential for cardiovascular assessment, yet current methods require invasive catheterization. T2-based cardiac magnetic resonance imaging (CMRI) enables non-invasive O2 quantification, but deep learning automation is constrained by scarce annotated data. We propose a unified self-supervised learning (SSL) framework integrating cine CMRI and T2 oximetry CMRI to learn generalizable representations without labels. Our approach pre-trains ResNet and vision transformer encoders using contrastive learning and masked image modeling on over 48,000 cardiac images. Pre-trained encoders are fine-tuned for O2 saturation regression with uncertainty quantification to enhance clinical trustworthiness. Our SSL framework significantly outperforms traditional radiomics and supervised baselines, with SimCLR pre-trained ResNet achieving a mean absolute error of 3.70, representing over 15% improvement. These findings demonstrate SSLs potential to address annotation bottlenecks in non-invasive cardiac diagnostics.
From the RadAI FDA Approvals Database
Time IS Brain, S.L.
BraiN20® (BraiN20)
BraiN20® is a portable, non-invasive medical device that helps clinicians monitor neurological status by recording and analyzing somatosensory evoked potentials (SSEP), specifically the N20 cortical response. It stimulates and records electrical signals in real-time, providing objective data on nerve function, which assists in neurological monitoring during clinical assessments.
Honeynaps Co., Ltd.
SOMNUM (SOMNUM)
SOMNUM is an AI-enabled software application designed to assist physicians in diagnosing sleep and respiratory-related sleep disorders by automatically analyzing polysomnography (PSG) data. It uses artificial intelligence algorithms to detect sleep stages, arousals, respiratory events like apnea, and periodic limb movements, allowing for efficient sleep study interpretation and report generation.
Silony Medical GmbH
VERTICALE® Navigation Instruments
The VERTICALE® Navigation Instruments are surgical tools designed to help surgeons accurately locate anatomical landmarks during spinal surgeries, especially in minimally invasive procedures. They work with third-party surgical navigation software that uses imaging like CT or MR scans, improving surgical precision and patient outcomes.
The Sharpest Insights, Effortlessly
Save Time
We scour dozens of sources so you don't have to. Get all the essential information in a 5-minute read.
Stay Informed
Never miss a critical update. Understand the trends shaping the future of your practice and research.
Gain an Edge
Be the first to know about the tools and technologies that matter, from clinical practice to academic research.
Ready to Sharpen Your Edge?
Subscribe to join 11k+ peers who rely on RadAI Slice. Get the essential weekly briefing that empowers you to navigate the future of radiology.
We respect your privacy. Unsubscribe at any time.